




Insight
Recession is looming, but it’s not all bad for femtech start-ups
Although opportunities in women’s health accelerate, investors remain cautious

As the International Monetary Fund (IMF) is signalling the unofficial start of recession, digital health funding slows amid investment uncertainty.
The past six months have brought new challenges for both investors and entrepreneurs. With higher-than-expected inflation, global financial conditions are becoming tighter and the world economy is on the brink of facing one of its weakest years since 1970.
The outlook for the global economy has “darkened significantly” in recent months, said IMF chief, Kristalina Georgieva, predicting a tough 2022, and an “even tougher 2023”.
IMF officials announced that inflation was higher than forecast with prices in the US raising at a 40-year high of 9.1 per cent in June. In Britain inflation has jumped from almost zero during the pandemic to 9.1 per cent and is expected to top 11 per cent by October.
Although modest inflation can be attractive to consumer goods companies, very high inflation rates could make planning and investment decisions harder, analysts say.
Femtech has been a growing area of interest with funding reaching US$2.5bn in December 2021. However, experts believe that investment in the buzzy sector will slow down.
“Femtech is still a very immature market in many ways,” says Becky Warnes, business consultant and NHS advisor. “Getting tech into health systems is going to be very difficult for all start-ups, but particularly for those in femtech.”
According to data from the venture fund, Rock Health, digital health start-ups banked over US$29.1bn in 2021, but femtech companies enjoyed three per cent of the funding.
“Women’s health is a very specific investment vertical,” says Priya Oberoi, angel investor and founding general partner at Goddess Gaia Ventures. “However, women are starting to realise the need for differentiated health care and the demand is going up.
“We are in an era where entrepreneurship has been slightly glamorised and for that reason alone, more start-ups and entrepreneurs will emerge. The process will remain the same. What is going to change is the speed of the investment.”
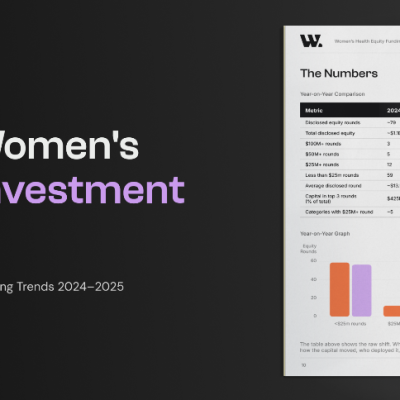
Indeed digital health funding fell in the first half of 2022, according Rock Health, suggesting that a drop in funding could be caused by start-ups looking to trim costs and reduce positions.
The report has shown that investment fell significantly in the first quarter of 2022, with digital health start-ups raising US$6bn compared with US$7.3bn in the fourth quarter of 2021.
The funding slowdown means the environment is shifting and start-ups need to learn how to navigate the new economic landscape and adapt to competition.
“Investors will be willing to invest where there’s historical return on their investment and where there is going to be a real profit,” says Warnes.
“Femtech has certainly many values-driven driven businesses, but I think when it comes to putting money on the table, investors will look for start-ups with valid solutions to valid problems.”
For Tess Cosad, former research analyst and founder of the London-based femtech start-up, Bea Fertility, the economic consequences of the pandemic are complex.
“At the seed stage, we are all having to figure out how to contend with smaller rounds, lower valuations and longer runway.
“Any business that was going to take longer to get to profitability is now going to struggle to raise more capital. There is definitely potential for some incredible companies to come out of this and I’d love to see more investors ‘taking a risk’ and backing more women’s health companies.”
Oberoi advises entrepreneurs to start talking to investors earlier on.
“Make sure your pitch deck is very clear and that your lexicon illustrates what you are trying to solve with much more clarity. Find out what’s the economics of solving those problems and use those statistics to build a global picture.
“Start-ups are doing a brilliant job. Now they need to adapt and think more carefully about their numbers, their unit economics and ultimately, about what they are trying to achieve.”











Black women in the UK want clearer, more accessible breast cancer screening information, research has found.
The study looked at why Black African and Black Caribbean women are less likely than white women to attend breast screening.
Researchers at the University of Surrey held focus groups and interviews with 47 Black African and Black Caribbean women aged 50 to 71.

Women in this age group are routinely invited for NHS breast screening.
The researchers said only 45 per cent of Black women attend screening, compared with 63 per cent of white women.
Anietie Aliu, lead author, postgraduate researcher at the University of Surrey and registered nurse, said: “Diagnosing breast cancer early can dramatically improve a person’s chance of survival.
“Breast cancer screening plays an important role in this by identifying the cancer and ensuring a person receives speedy treatment.
“Despite the importance of screening, Black women are less likely to attend appointments than white females.
“This puts them at risk of a potential cancer being diagnosed late and spreading to other areas of the body. We need to understand what is preventing Black women from attending these appointments and help identify ways to remove such barriers.”
The study found a need to increase awareness of breast cancer screening, especially among women less familiar with the service.
Some women, particularly those born outside the UK, knew little about breast screening before receiving their first invitation.
Others questioned why they needed screening when they had no symptoms.
The importance of trusted conversations was also identified.
Researchers found that some Black women expected their GPs to speak to them about breast screening, particularly before they reached screening age.
Although NHS breast screening is organised through national screening services, researchers said GPs often have established relationships with patients and may be well placed to offer brief advice on preventive care, including breast screening.
Participants called for stronger links between GP practices, breast screening services and Black community champions.
They said this could help women receive trusted information, ask questions and feel reassured.
Faith and religious beliefs also shaped decisions for some women.
Some Black African Christian women said illness, including cancer, was not permitted by God in their bodies, while others saw screening as a personal choice that did not conflict with Christian faith.
Muslim women highlighted the importance of being able to state their religion on medical appointment forms to help ensure they were seen by a female mammographer.
A mammographer is a healthcare professional trained to carry out breast screening scans.
Aliu added: “Breast screening can save lives, but our findings show that attendance is shaped by multiple factors, not just awareness, although awareness remains important.
“Women need relatable screening information, reassurance, flexible appointments and services that are accessible within their communities.
“Many felt that invitation letters were too formal, and that leaflets and media imagery did not reflect them, making it harder to relate to screening.”
Dr Afrodita Marcu, senior research fellow at the University of Surrey and member of the research team, said: “We need a more collaborative approach, where primary care, screening services and community voices work together to support women before, during and after the invitation.”
The researchers said future breast screening interventions should be designed with Black women, rather than for them.
They said user-friendly and culturally relevant resources, developed with communities, healthcare professionals and screening services, could improve understanding, reduce fear and make breast screening feel more accessible and reassuring.
Dr Robert Kerrison, associate professor of cancer care at the University of Surrey, said: “There is no question that breast screening can be lifesaving, but we need to make it easier for women to understand, access and feel reassured by the programme.
“This means improving communication, addressing practical barriers and making sure healthcare professionals and community partners are supported to provide clear and trusted information.”
The team has also explored healthcare professionals’ perspectives and worked with stakeholders to develop user-friendly materials with Black women.
Researchers said this co-designed approach could help ensure breast screening messages are culturally relevant, practical and shaped by the people they are intended to support.
Insight
“Women’s voices should be heard and pain should never be ignored,” says Wales’s first Women’s Health Minister

Women’s pain should not simply be endured, Wales’s first women’s health minister has said.
Delyth Jewell said she was determined to tackle the normalisation of pain in women’s healthcare and ensure women’s voices are listened to.
Speaking during a Women’s Health Summit at the Temple of Peace on Thursday, July 16, she said: “For too long, women’s health has been treated as an afterthought. No woman should be afraid to speak up about pain or things that don’t feel right.

“Women should be believed about their bodies, and I am determined to change the culture that has let too many women down.”
She added: “Women’s voices helped create the Women’s Health Plan. Now we’re making sure those voices continue to shape what comes next.”
The summit brought together clinicians, researchers and women with lived experience to tackle the normalisation of pain in healthcare and identify how women’s voices can better shape NHS services.
Lived experience means insight from people who have personally gone through a health issue or used healthcare services.
The event focused on pain linked to clinical procedures and long-term health conditions, drawing on research evidence, clinical expertise and women’s personal experiences.
Following the summit, minimum standards for service user engagement will be drafted to ensure women’s voices continue to influence the delivery and future priorities of the Women’s Health Plan.
Service user engagement means involving people who use health services in decisions about how care is designed, delivered and improved.
Work will also begin to refresh and strengthen the plan, including gathering feedback directly from women across Wales.
The NHS Wales Women’s Health Plan was developed after discovery work in 2022, when women across Wales shared their experiences of healthcare.
Many said they had not felt listened to, had symptoms dismissed or had lived with pain for years before receiving a diagnosis.

Hosted by Amanda Ducach, CEO, and Morgan Rose, chief science officer, EmaEQ
Healthcare companies have spent the last two years hearing the same advice: get AI into your product. Few have been told what that actually takes.
Most default to the fastest option. Plug in a general-purpose model, wrap it in a chat window, and call the box checked. It looks like progress on a roadmap slide. It rarely holds up once a real patient is on the other end of it.
We’ve spent years building AI specifically for healthcare, and the lesson that keeps repeating itself is simple: accuracy is not the same thing as trust, and trust isn’t something you bolt on after launch. It has to be part of how the system is built from the first line of code, not a feature added once regulators or users start asking questions.
That distinction is the whole reason clinical accuracy gets treated as a checkbox instead of a discipline. A model can sound confident and still be wrong in ways that matter enormously in a health context.
Knowing the difference, and building for it deliberately, is what separates AI that’s genuinely safe for care from AI that’s simply fast to ship.
On July 20th, we’re hosting a live conversation about exactly this: what companies should be paying attention to before they choose an AI to build with, what clinical accuracy really requires, and the pillars we hold every AI system to before it gets anywhere near a patient’s care.
The Healthcare AI Playbook Webinar: July 20th, 1:30-2pm EST, live on LinkedIn.
Register here: https://www.linkedin.com/events/7482643171823509504?viewAsMember=true
If your team is building anywhere near healthcare, or evaluating what’s already in your product, this is the conversation we think the industry needs right now.








 Insight2 weeks ago
Insight2 weeks agoWomen with PMOS should have annual NHS checks, new guidance says

 Diagnosis1 week ago
Diagnosis1 week agoTwo “gamechanger” tests set to speed up endometriosis diagnosis on the NHS

 News3 days ago
News3 days agoNew menopause drug approved for use by NHS in Scotland

 Cancer1 week ago
Cancer1 week agoThousands of women could avoid painful cancer exam with new AI blood test

 News2 weeks ago
News2 weeks agoBreast cancer biosensor and low-cost ultrasound startups win women’s health AI competition

 Entrepreneur1 week ago
Entrepreneur1 week agoApplications open for the third W Accelerate with Merck KGaA and M Ventures

 News2 weeks ago
News2 weeks agoClue spotlights seven women’s health journeys in new campaign

 Fertility1 week ago
Fertility1 week agoOlder women face lower chance of fertility treatment working, even with donor eggs, study finds